
7 |La consommation de mangues et la vulnérabilité de la santé des enfants dans la périphérie nord-ouest de la métropole de Douala
Mango fruit consumption and children
Mots-clés:
Vulnérabilité| santé des enfants| consommation| fruit de mangue| périphérie| Douala|Résumé
Le présent article pose le problème de la vulnérabilité des enfants face à la consommation des mangues non mûres, trop mûr et des mangues infectées en insistant sur la qualité et la quantité consommée. Le but de ce travail est de comprendre pourquoi les enfants sont plus vulnérables aux maladies après la consommation de ce précieux fruit dans la banlieue Nord-ouest de la métropole de Douala. Une méthodologie pluridisciplinaire a été adoptées, les données primaires et secondaires ont été collectées et traitées à partir des techniques quantitatives et qualitatives. Les résultats révèlent que ces enfants, pour la plupart, ne respectent pas les principes d’hygiène de base, il y’a un manque de suivi des parents, les anticorps ne sont pas bien mature pour résister à certains pathogènes et l’ignorance aggravée. Un plan d’action en synergie avec interconnections accompagnée par des ressources humaines et physiques pourraient résoudre ce problème considérablement.
Introduction
Mangifera Indica L, also known as mango is a member of the plant family Anacardiaceous, order Sapindales, class Magnoliopsida, division Tracheophyta (vascular plants) and scientific name Irvinga Gabonensis. The species name is Mangifera Indica which means “an Indian plant bearing mangoes” (Indu Mehta, 2017, p. 20-24). Mango as seen by Vavilov (1926, p. 16) originates from India precisely in Indo-Burma region following observations made on the genetic diversities. Today, more than 1000 species exist in the world. In the same light, mangoes have been cultivated in South Asia for thousands of years while cultivation began in South East Asia only between the 5th and 4th Centuries B.C. According to Purseglove 1969, it was only during the 10th Century A. D. that the Persians carried it to East Africa and during the 16th Century A. D. the Portuguese brought it to West Africa and later spread it to African countries like Cameroon. As such, mango stands as the world’s third largest food crop (M. Elhadi Yahia, and al., 2019, p. 36-42).
Suburbs of most cities in the developing countries are often rich fruits production haven that readily feed the cities. The city of Douala and its suburb are not an exception to this practice. Fruit cultivation in the suburbs is not only meant to feed the cities but the local populations as well, since their welfare depends on the sector. Fruits consumption in the suburbs of Douala is not regulated by the local stakeholders; this places the vulnerable population at risk of disease infection after consuming unripe, overripe and unwashed mango (Moby Etia 2017, p. 6-7). This practice becomes challenging to the health of the population and children in particular because they represent a significant portion. Moreover, reports from the Regional Delegation of Health for the Littoral (2018, p. 6-8) support the view that the consumption of unwashed fruits exposes the children to disease infections like stomach-ache, cholera, diarrhoea and dysentery etc.
Basing on the findings of M. E. Nkumbesone (2017, p. 3-7), within the past twenty years, this study area was mainly made up of the indigenous populations such as the Abo in the Bonaléa Sub-Division and the Bakoko in Dibombari. Presently, the phenomenon of suburbanisation and demographic explosion coupled with mass rural exodus and migration has transformed the area to becoming highly heterogeneous. This population growth is clearly seen in the rapid explosion of the youthful age group (6-12 years) which is affected after consuming unripe, overripe and unwashed mango. Considering that mango contains 12.6% sugar content (Agbor Ebai and al., 2018, p. 52-57), it attracts flies and other disease carrying vectors. When children now consume these unwashed fruits, they become vulnerable to disease infections. Children aged less than 14 represent a significant portion of the entire population of 43%, youths 52% while the aged total five percent. These statistics reveal that close to 50% of the population is vulnerable to disease infection during the mango season. This has been proven by the increased number of children admitted in health centres and suffering from infections related to mango consumption and as well as from clinical reports. Basing on the fact that the children are more prone to disease infections than the other age groups and given that they are very mobile (gathering mango from one place to another), disease infection and contamination finds a fertile ground among them. Some of whom go in search for mango in more than one kilometre.
Reports from consultation books in some hospitals and dispensaries within the study area showed that; of 1100 patients received in these health units after mango season, 670 were children (60.9%) in 2017, of 920 patients in 2018 after the mango season, 713 were children (77.5) and of 830 patients in 2019, after the mango season, 711 were children (85.7), with principal illnesses being diarrhea, dysentery and fever (F. M. Wendy, 2020, p. 40-43).
Now therefore, the problem is why the children are most vulnerable to disease infection after consuming unripe, overripe and unwashed mango? In the same light, this paper questions the laxity of stakeholders in not controlling the children’s consumption rate of mango which has led to exposure to disease infection. The objective is to analyse the children’s health vulnerability to disease infections after consuming mangoes within the study area.
Méthodologie
1. Methodology
1.1. Presentation of the study
Douala is located in the South Western portion of Cameroon, under the territorial delimitation of the Littoral region. The study area from Bonaberi to Souza is located between two Divisions within the Littoral Region. One of them is the Wouri Division that harbours Bonaberi and its environs while the other is the Mungo Division harbouring Souza and its environs. Located between latitudes 4º25´ to 3º99´ N and longitudes 9º50´ to 9º76´ E, the study area is mostly rural and suburban. Bounded to the north by Mbanga and Yabassi Sub-Divisions, west by the Atlantic Ocean and to the east by the River Wouri and part of South West Region. The study area is comprised of three Sub-Divisions namely; Douala IV, Dibombari and Bonaléa (Map n°1).

1.2. Data collection
This study made use of the hypothetical deductive methodology proposed by Leibniz which consists of validating hypothesis from observation. The general method adopted is the geographical method of investigation which comprises of four stages: Observation, Description, Analysis and Interpretation of facts and phenomena in the society. It also privileged the trans-disciplinary approach of research and eco-health approach which analyses the relation between humans and environment.
Data exploited within the framework of this study were collected between the months of February and September which represent the start of harvest and the end of harvest. The aim was to have sufficient facts on the consumption of mangoes within the study area. Qualitative data were collected through observation (in situ observation and participating observation), by observing children gathering and consuming mango, those admitted in local health centres and at home; and interview (direct and indirect interview) with parents and health personnel.
On the other hand, quantitative data were collected through survey. The study area was sampled using the quinary method of investigation (G. Biyogo 2005, p. 65-66). The survey was carried out with a total of 250 questionnaires administered in respect to some geographic, socio-economic, socio-cultural, socio-political and sanitary criteria of the area. Out of the 250 questionnaires, each community received a total of 50, to determine the rate of quantitative representation. Random sampling was applied in accordance to centre-periphery, demographic composition and social amenities of the area. The questionnaires were conducted on different field trips to some five communities (Fiko, Dibombari, Bonaléa, Souza and Bonaberi) which in 2015 registered 437.849 inhabitants (BUCREP, 2015). By application:
-
H: total number of households sampled=250 households
-
P: total number of population in the sampled area=437,849 inhabitants
This therefore gives:
![]()
Given the rate of application of 5.7% which is more than the five percent conventionally retained; we can therefore conclude by saying that the quantitative choice of representation is satisfactory.
In all, primary data were collected on the field while secondary data were collected from libraries (University of Douala) and from archives (Bonaberi District Hospital and other health centres, DUC).
1.3. Methods
The study used two types of questions and data in the questionnaires. The first set of questions were fixed choice questions in which the informant had to choose an item amid several modalities, it is equally in the form of “Yes” or “No” questions. On the other hand, the questionnaires had open-ended questions which permitted the informants to freely give their views on the vulnerability of children from the consumption of mango fruits. This exercise permitted the codification of responses from both questions types and later expressed as percentage for a better interpretation.
Secondly, the qualitative data were analyzed with the help of MACTOR software to evaluate the various roles of the actors (fig 2 and 3) within the framework of this study. It equally helps to analyze the most vulnerable strata of the population from the consumption of fruits. On the other hand, quantitative data were treated with the help of SPSS, Excel 2007 and QGIS, Philcarto and Phildigit.
These processes have led to establishing the interrelation between the actors, given that the software played a specific role. SPSS 21.0 permitted to analyze socio-demographic data on the vulnerability of children from mango consumption, Excel 2007 granted access to further analyze data from SPSS and draw appropriate illustrative graphs. QGIS, Philcarto and Phildigit were used to locate the study area which ended with the production of a location map of the study area.
Résultats
2. Results and discussion
2.1. The pre and post harvest periods of mango
The town of Douala which happens to be the economic capital of Cameroon experiences increase in population size from within and out of the country as well as increase in economic activities. The littoral region of Cameroon witnesses increasing cultivation of food crops and cash crops to meet high demands in the cities. The cultivation of mango in the suburbs of Douala is not often in large scale and intensive manner. Unlike other regions of the country, planting of mango in the littoral region begins in the month of June and extends to August (the end of June and August) due to the availability of water to permit plant grow healthy. Pre-harvest factors such as light, temperature, carbon and water availabilities affect plant growth.
Fruits cultivation thrives well in the area as a result of favourable physical and human factors ensuring the cultivation and production processes (A. Y. Onaolapo and al., 2019, p. 8-9). The equatorial climate which is hot and humid (26.8 °C/year; 4000 mm/year) and dominated by the monsoons in the second half of the year favours fruits cultivation. Moreover, this area records an average rainfall of 230 days and relative humidity of about 93%. This prevailing climatic condition sets the pace for the growth of fruits. The hydromorphic and sandy-clay soils are enriched by chemical fertilizer which affects human health when invariably applied. Upkeep is done continuously as the plant grows to maturity.
Harvest begins at the end of February and the start of March. The peak periods are the months of May and beginning of June. Generally, the rural areas are very remarkable in terms of mango production; this can be explained partly by the availability of sufficient land areas and man-power. Villages situated between Bonaberi to Souza are good production areas. Production, and commercialization of mango in this geographic area is mainly informal, and its consumption obeys to no hygiene and sanitation principles. This explains why the children become vulnerable to disease infections after random eating of mango.
The local producers have multiples choices to make on where their goods should be sold and consumed. Middlemen quickly get into scene by supplying to Biotropical Company for processing, supplying to other neighbouring towns, while the local population and the children in particular consume the rest. Mangoes consume by the children are mostly unwashed overripe or unripe which falloff during storms and the absence of their parents and local authorities on the scene sets the pace for the practice.
2.2. Factors of health vulnerability linked to the consumption of mangoes
It is however unfortunate to know that most of the data on the number of infected children are not available in recognized public and private institutions within the area of study but most are found in clandestine and the informal sectors. The Dibombari district hospital for example and its health zones (Bomono, Souza, Nkapa, Boadibo,…) register few cases, confessional hospital mostly found in Bonaberi also register very few cases. The absence of data from these aforementioned health institutions is an indicator of the weakness in providing health care to the population. The district hospitals are deserted by medical personnel and are constantly experiencing shortage/absence of drug supply. Also, the actions of community health agents are not visible in the different localities.
The reports from the clinicians attest that the children are most vulnerable to disease infections after consuming a fruit suspected of having a pathogen. The same information was collected from patients who presented their hospital cards and in them were written consumption of mango as the suspected cause of their ill health. During consultations, clinicians discuss with patients and parents who explain the type of food consumed during the previous days, added to this are symptoms of diseases related to unripe, over-ripe and infected mangoes consumption which were visible. Though some children may be allergic to mango consumption, this does not in any way contradict the fact that the children are most vulnerable to disease infections from infected mangoes, unripe and over-ripe and unwashed mangoes. Investigations revealed that close to 80% of the children suffered from diseases related to mango consumption either from infected ones, unripe, artificial ripe, over-ripe unwashed or from excesses. According to V. A. Palejwala (1984, p. 255-262), the degree of ripening increases the rate of infections in mangoes and A. R. Ajayi and G. O. Mbah (2007, p. 60-66) added that the usage of Calcium carbide can induce ripening within 24 hrs. Since this chemical product is less expensive, some traders go for it to enable ripening. Graph n°1 presents percentages of children vulnerability from the consumption of mango.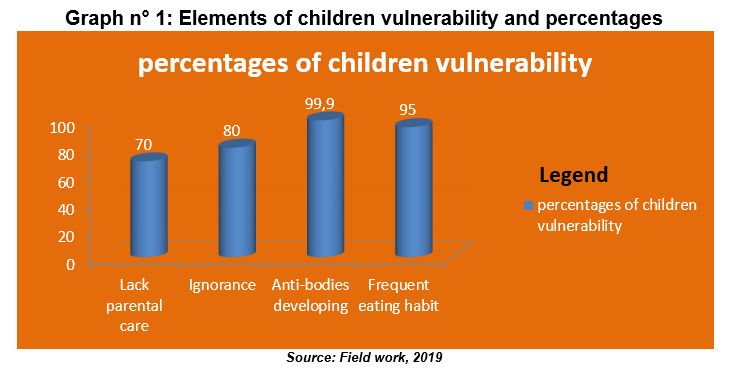
Graph n°1 presents factors of children vulnerability by outlining the fact that in most cases, parental care is absent, parents often go about their businesses and other occupations while other simply lack time and some are just ignorant. The results revealed that 70% of the children lack parental care, ignorance totalizes 80%, developing anti-bodies and frequent eating habit stand at 99.9 % and 95% respectively. These statistics brings to light children’ health vulnerability and disease infection observed on the field of study. The four aspects identified and listed on graph n°1 are among the root causes of children vulnerability and igniting disease infections on the children. Closely linked to these factors is poverty which is at the foundation. Actually, the parents most at times do not wilfully abandon their children at the mercy of disease infection but they are been driven by poverty to go in search for food. More than 95% of the local population lives below the poverty line and they are from a typical African family setup characterised by many children and extended family structure. This socio-cultural framework makes it difficult to families to have better living standards. The consumption of mango as a meal during this period is common-place. Since the mango trees are widely distributed within the study area, there is random gathering and eating by the children which exposes them to disease infections. Ignorance of local stakeholders to control the children from entering and collecting unripe and overripe fruits from the bushes also exposes the children to disease infections.
2.3. Epidemiological repercussions linked to the consumption of mangoes
Mango provides amazing advantages to human populations such as constituting a rich source of Vitamin C which aids the immune system of the body; it helps in keeping cholesterol in check and increasing fertility. On the economic plan, it provides revenue to the actors engaged in the practice (O. A. Kouassi 2012, p. 22-43). However, mango does not only provide outstanding advantages to the local populations, reason for which it is said to be a ‘mixed blessing’. In case of excess consumption and lack of precautions, it can lead to health effects that may entail huge amount of money to remedy the situation or in some cases, it can lead to death of the victim (H. Kante-Traore and al., 2017, p. 13-21). Though the local population often links the cause of death to be from witchcraft manipulation and this conception is often generational. It is supported by the strong attachment to cultural values which in most cases prone to negativity.
Though majority of the inhabitants cherish the fruit, they are however misled by their passion to eating the fruit without careful examination of the quantity and quality to consume. As a result, the quantity, quality of fruit and the frequency of consumption become a major health challenge. Field investigations show that on average, eight children out of ten consume between 15-20 mangoes per day during the peak periods. This quantity consumed however, varies with the children ages and the length of production season. Table n°1 present’s statistics on the quantity of mango consumed during the harvest season according to age groups selected for the study.
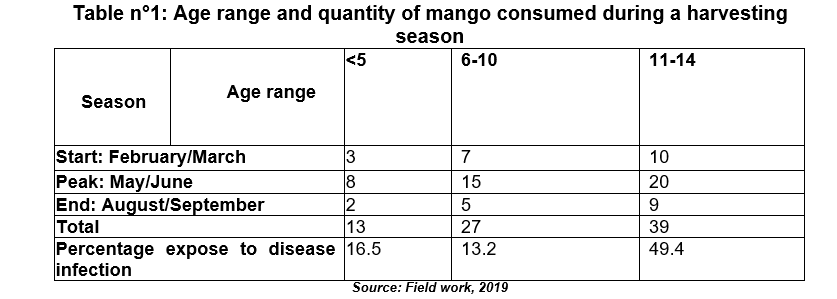
From table n°1, the quantity of mango consumed varies with the age group. Generally, children age less than five usually consume on average three mangoes per day (03/day) at the beginning of the production season, consumption doubles and at times triples during peak periods due to availability of mango and later falls progressively with time to two mangoes per day (02/day). The same principle is applied to the two age brackets, that is, those ages between 6-10 and 11-14. When comparing the first and the last stages in a season, it is realized that the first stage override the third stage in the total number of mango consumed simply because, the populations have for long been waiting on harvesting to start. The peak periods usually record outstanding number of mangoes consumed which on average are 8, 15 and 20 corresponding to the age of less than five, 6-10 and 11-14 respectively. The above percentages reveal that close to 79% of the children are exposed to disease infections after consuming mangoes during harvest season.
One of the main problems facing many communities and individuals today is that of respecting established conventional norms (I. Mwamba, 2018, p. 216-222). Just like many other sectors of the economy whereby, respecting international norms is seen as a taboo, the sanitary measures to be implemented in the consumption of mango is lacking (C. Mbungu and al., 2016, p. 947-953). Field works revealed that children are highly ignorant of the fact that excessive consumption can lead to adverse effects in their body. Excessive consumption of mango by the children in this field of study is explained partly by the presence of many mango trees and their capacity to produce much fruits per season. The high production and consumption rates of mango are further explained by increasing number of trees as a social livelihood of the actors. In Bomono Ba Mbengue and in Nkapa, two out of five children age between 13 and 14 confirmed of haven consumed up to 30 mangoes per day during peak period. The informants also acknowledged that they at times eat mango in excess when they are betting on an outcome, this often pushes them to eat the fruit in excess. Unfortunately, their desire and appetite to eat much fruits do not usually tally with the body demands; thus, such situation often leads to body disorder and disease. Graph n°2 represents evolution of quantity of mango consumed per day during a production season and the number of victims who were infected after eating excessively.
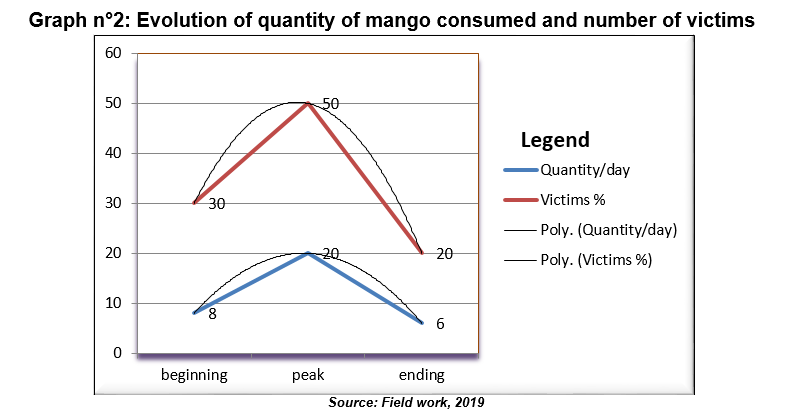
Basing on the facts and figures in graph n°2, the first thick blue line represents evolution of average consumption of mango per day as the season unfolds beginning from 8, 20 to 6 mangoes. In the same light, the number of victims represented by the red line and expressed as a percentage progresses with increase consumption. The last two tiny black lines simply denote the evolution and the link between quantity consumed and number of victims. It is clear from graph n°2 that as the number of mango consumed per day increases, the number of children infected increases as well. From table n°1 and graph n°2, there exists a positive correlation in the consumption habit of children during the mango season which makes them vulnerable to disease infections. Graph n°2 also exposes the relationship in the vulnerability of children toward infectious diseases upon daily consumption of mango and number of victims.
Closely linked to the problem of quantity is that of quality. As observed, the children just like the other age groups do not really consider the quality of food to be consumed but rather focus on the quantity and the desire to fill their stomach. Majority of the population ravaged by economic constraints and persistent low standards of living have forgotten the notion of quality in their dietary. The basic notions of hygiene and sanitation have completely been wiped out in the society at large due to ignorance, minimization of risk and socio-cultural believes. Although some fruits cannot easily be infected while still attached to the tree due to the its protective agents, it is however important to note here that disease vectors like insects and births can piece the fruit and inject toxic substances which result to progressive rotting of the fruit. Maggots, micro and macro organisms and other insect larva would definitely colonize such fruit thereby rendering it highly risky for consumption. The children out of negligence and hunger do not usually pay attention to these health details and of course, such practice sets the pace for disease infection. Such a situation can be described as a stubborn fly follows the corpse to the grave.
A test conducted based on the probability of infection of mangoes gathered on the ground after a period of 48hours and using three mangoes drawn at random from a set of ten mangoes. Mindful of the fact that the probability of infection P (I) always lie between zero and one, that is,
0 ≤ P (I) ≤ 1; and applying the complementary events method to prove that at least one mango is infected gave the following:
P = Probability I = Infection I?= No Infection
Generally, P (I) = 1 – P (I?)P(at least one infected) = 1- P(at most zero infected)
By application; P (1I) = 1 – P (I? I? I?) P(1I) = 1–0.99 or 99%
The above calculation based on the probability that at least one mango out of three drawn at random from a set of ten mangoes would be infected is valid because the result gives a very high probability (0.99) which is approximately one. The selection was highly unbiased, on different intervals and the same test conducted to some other mango trees around gave approximately the same outcomes. This therefore confirms the idea that when children gather mangoes on the ground without considering the probability of infection and the number of days it has been lying on the ground, they would be more vulnerable to disease infections. By induction, the idea of probability of infection conducted to some mango trees in an unbiased manner can tie squarely to the entire locality from Bonaberi to Souza since the test equally considered the notion of centre-periphery and socio-cultural features of the study zone.
Furthermore, such situation of high probability of infections coupled with lack of parental guidance, no proper home education and morals makes the children to be most vulnerable to disease infections. Investigations revealed that most parents in the area lack sufficient time to educate their children by letting them know the health dangers surrounding the consumption of unripe, overripe and unwashed mango or even consuming in excess. It is usually practice and a lifestyle for the children vagabonding the streets, villages and bushes in search for mango during production season. At this point, they eat the precious fruit at random without paying least attention to the quantity and quality consumed.
Most often, children leave the schools during break period and go in search for mangoes to eat and even after classes; they spend more time on the way searching for mango before arriving home. It is quiet unfortunate that during these outings, their primary objective is to fill the stomach from hunger and do not really care of being infected. Infection is very possible at this stage because they do not border to wash the fruits before consuming and equally pay less attention to the quality of fruits. This view is in line with the suggestions of Z.N. Fogwe, N. Nzonkwo Tetchaa (2015, p. 95-112), who advocated that insanitary conditions are gate to disease infections in any given territory.
2.3.1. Some selected diseases affecting the children
This paper equally seeks to have profound knowledge on the most recurrent diseases affecting the children after consuming mango. This is so because in reference WHO (2009), the protection of our diet from hazards must be considered one of the essential public health functions of any given country like Cameroon. Now, basing on the strength of the results of investigations from health personnel and the populations, a summary of illnesses were recorded within the context of mango consumption.
Diarrhea. This is the most common disease which about 90% of the children suffered. According to Mohammed Wasim Siddiqui (2010, p. 4-8), artificial ripening of mango is a threat to human health just like the unripe mango. Eating too much mango can easily over-stimulate the intestinal wall, which further increases bowel movement frequency leading to loose stools and diarrhea. The children are the most vulnerable because they go around eating mango without paying attention to the quality and quantity consumed so, this often leads to diarrhea. Since their metabolism cannot withstand great quantity and the fact that they might have consumed infected mango. This is very possible because about 95% of these fruits are gathered on the ground, 20% of mango which fall on the ground are usually pierced, this of course ease excess to bacterial which finally contaminate the fruit. About 10% of the fruits were already pierced by birth and insects before touching the earth surface. Added to this is the fact that domestic animals like cow parade the localities of Bekoko and Bomono Ba Mbengue littering the entire zone with excreta; dogs, goats, fowls and other domestic animals are not left out in the matter of contaminating the environment since a vector may transmit a disease from one point to the other (E. W. Ejuande and al., 2017 p. 305-337).
Furthermore, the reports from clinicians and patients’ booklet show that the children are most vulnerable to dysentery infections caused by a parasite, a bacterial or a protozoan which is susceptible of originating from a previous consumption of unripe, over-ripe or infected mango.
Stomach-ache: Naturally, unripe fruits like mango are not easily digestible and chewing them is not all that easy. Such fruits require considerable energy to ease the digestion processes which usually take a relative longer period of time. The children usually lack patient to chew the fruit properly before swallowing, the lack of patient pushes the children to swallow the fruit prematurely which later constitutes a serious problem to the stomach as the organisms would have to bear the effect of impatient; thus, leading to stomach disorder. Just as C. Ndi Amuoh (2011, p. 3-5) advocated, in cases where chemicals were used, it would have a negative reaction in the body. This idea equally sustains the fact that stomach ache in children is caused by the presence of chemical substances in mango which were applied either to facilitate growth/production or ripening/conservation.
Bloating: This usually results from unripe fruits which are actually less digestible because they have not yet undergone the natural ripening process that makes their nutrients and the fruits are yet to be edible. This can be explained by the fact that unripe fruits usually contain more complex carbohydrates that are harder to digest like starches that are more resistant to digestive enzymes. Moreover, unripe fruit basically lack the natural ripening process that helps in breaking down fibre and other elements. So, this makes the children suffer from bloating and other related illness.
Generally, indiscriminate eating of mango would mean that the children are liable to consume fruits grown both naturally and artificially. This of course is dangerous because human exposure to chemical substance intake and nutritional imbalances are known or suspected to be involved in causing cancer, cardiovascular disease, kidney and liver dysfunction, hormonal imbalance, reproductive disorders, birth defects, premature births, immune system suppression, musculoskeletal disease, impeded nervous and sensory system development, mental health problems, urogenital disease, old-age dementia, and learning disabilities. Moreover, according to Hossain, M. F. Akhtar and M. Anwar (2015, p. 1755-1760), among these disorders and diseases some might be attributed to the exposure of human body with harmful chemicals used in food items. Jayan (2011 p. 37-63); Hakim and al. (2012, p. 247-251) argued that the regular consumption of artificial fruits leads to dizziness, weakness and body ulcer
2.4. Socio-spatial responses of various actors to the health effects
This paper also seeks to know the efforts and the reactions from different actors toward the health effects resulting from the intake of infected mango while laying more emphasis on the local population. As noted from the preceding paragraphs, the effects are not felt at the same magnitude in all the villages and as a result, the socio-spatial responses vary. The socio-spatial responses vary from one locality to the other and from one household to the other depending on the level of awareness, socio-cultural believe and socio-economic status. The main stakeholders identified are: Douala urban council, Douala IV, Dibombari and Fiko local councils, phyto-sanitary brigade, health personnel, local populations and NGOs. The number of stakeholders present in the area is more figurative for statistical purposes than the actual number involved in the struggle to eradicate health challenges resulting from mango consumption. Consequently, the analysis of actors interplay reveals absence of synergy and distant relation between stakeholders. Only the health personnel and the local populations are engaged in the struggle. Local councils are more concerned in collecting taxes from the sale of mango and in conflict resolution. Quarter heads and chiefs are well noted for conflict resolution in the community. Local churches and school also intervene either directly or indirectly in sensitising the population. As a result of negligence from stakeholders like the State and local councils, the populations take the bull by the horn in seeking panacea to health challenges. Graph n°3 presents socio-spatial responses of the populations to disease infections in the suburbs of Douala.
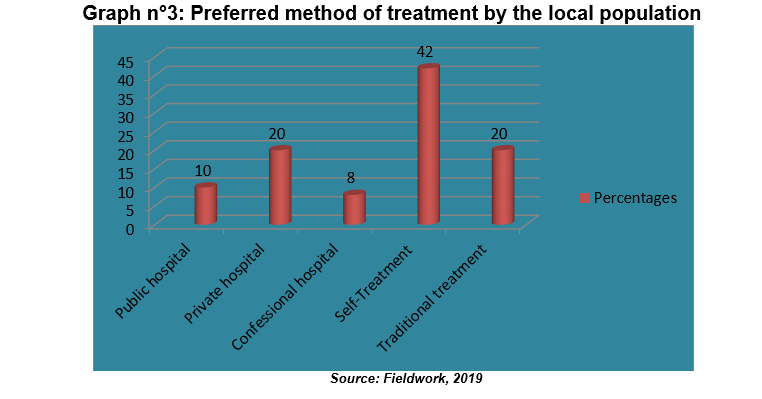
Graph n°3 represents realities uncovered in the suburbs of Douala. The public and confessional hospitals standout to be the least preferred treatment method, recording 18% patients suffering from infections related to mango consumption. On the contrary, self-treatment standouts as the most preferred treatment method by the populations and total 42%, followed by private and traditional treatment recording 40%.This situation is accounted for by the fact that majority have what they called easy-access to drugs from nearby chemist, drug hawkers, friends and family members. Once they suspect symptoms of diarrhea, dysentery, stomach-ache and malaria, they immediate apply procedures which are at their reach.
The traditional treatment was discovered to be preferable by the local populations especially in Nkapa because the population live close to nature. That is, they consume much of natural herbs and guava leave has been identified as a remedy to diarrhea. There has equally been remarkable increase in the number of churches in the villages and the populations (believers) believe in divine healing from the prayers conducted in these local churches. D. Meva’a Abomo (2015, p. 79-84) supported the idea that this informal and obscure treatment methods generally creates a serious problem of public health both at local and the national level which inevitable draws the attention of studies like this to be able to identify the grassroots problems. This practice still prevails in the 21st Century because the notion of health risk from food insecurity is not well assimilated by the majority of the populations who often minimize the health risk, ignore the possible consequences and even believe that there is zero risk.
Moreover, graph n°3 further reveals the degree of poverty and ignorance within the study area as the number of patients who prefer self treatment and use of natural herbs rather than going to recognised hospitals (public, private and confessional) for treatment. A combination of graph n°1 and n°3 shows children’s health vulnerability to disease infections after consuming unripe, overripe and unwashed mangoes, as well as the quantity consumed per day.
Conclusion
Conclusion
This paper is aimed at showing that the children are most vulnerable to disease infections from the consumption of mango due to their uncontrollable eating habit, reluctant and refusal to respect hygiene and sanitation principles and the fact that the quality and quantity of mango consumed is not of importance to them. Mango consumption is a mixed blessing when sanitary rules are not respected and therefore, presents more health challenges when considering the poor quality and excessive mango consumption.
The paper presents factors of children’s health vulnerability which are poverty, lack of parental care, poor eating habit, fragile anti-bodies and ignorance to be the root causes of their ill health. Basing on statistics gathered on the field, the results reveal that the children are most vulnerable to disease infections after consuming unripe, over-ripe and unwashed mango (see table n°1, graph n°1 and n°2). Statistics show that close to 70% of children are infected by disease related to mango consumption (diarrhoea, dysentery, stomach-ache, etc.) during harvesting season. In some cases, the children’s ill-health can lead to death but the local population often associates the cause to be witchcraft. This is explained by their strong believe on traditional values, superstition and the fact that the area is mostly rural.
In the meantime, the reaction of stakeholders like quarter heads, Chiefs, local councils, Divisional Officer and phyto-sanitary brigade is not felt in sensitising the local population on the ills of consuming fruits suspected of being infected. The vicious cycle of disease infection from mango consumption each harvest season is sustained by the failure of stakeholders to respond proportionally to the problem. This therefore pushes the economically deprived population to solicit alternate treatments which are often inappropriate, ineffective and have no scientific base. As such, the consequences are much and are felt on the economic, social and psychological plans.
This paper therefore proposes collective actions from all actors. All stakeholders in both private sector (population, groups, associations and elites) and public sector (council, hospital and other decentralized authorities) should work in synergy to see that this problem is lessened. Proper cleaning of the environment should be reinforced and domestic animals kept under control while implementing sanctions on defaulters. Moreover, collective participation of all actors together with further scientific research would considerably remedy the problem just as Mursalat and al. (2013, p. 6-12) outlined. Collective actions should also consider the recommendations of FAO which were outlined by the WHO (2003), stipulating that 400g is the minimum consumption of fruits and vegetable per day. As such, the recommendations should be respected by the local population.
Sensitization, prevention and control strategies should be developed and implemented by stakeholders especially the medical personnel who better master the health domain and equally have living testimonies of different victims they must have come across. Sensitisation should be reinforced by churches, NGOs and other social groups in order that the rate of ignorance would decrease. Sensitisation campaigns should focus more on the possible health risk from indiscriminate and random consumption of mango, preventive measures of disease infections, general hygiene principles and on the need to consult a health physician in case of any ailment. It should also be conducted before, during and after harvesting season of mango. First aid treatments should be made available and drugs supplied to local hospitals, health centres and clinics in time and at reasonable cost. This would reduce the stress of referring patients to the Dibombari district hospital, Bonassama district hospital or the CEBEC hospital. Also, the technical plateau and infrastructures should be improved in these health zones.
Références
Bibliographic References
AJAYI Rotimi. and MBAH Gordian ONYEBUCHUKWU 2007, «Identification of indigenous ripening technologies of banana and plantain fruits among women-marketers in South-eastern Nigeria». Journal of Agriculture Food Environment and Extension 6(2), p. 60-66.
AGBOR EBAI and al; 2018, Sucrose processing in fruit, the case of mango, MSc Thesis, University of Calabar, Nigeria, Department of Food Sciences, p. 52-57.
BIYOGO Grégoire. 2005, Traité de méthodologie et d’épistémologie de la recherche. Introduction aux modèles Gabon, l’Harmattan, p. 65-66.
BUCREP 2010: 3ème RGPH, Rapport de présentation des résultats définitifs du 3ème recensement général de la population du Cameroun, Yaoundé, volume 2, p. 35-41.
ELHADI YAHIA, 2019, « Postharvest Insects and Their Control in postharvest technology of perishable horticultural commodities», p. 36-42.
EJUANDE Emmanuel Wonomu. and al; 2017, «Determinants of epidemiology risks in hospital milieu of Douala: case of the New-Bell Health District», In: Dynamiques urbaines et Transformations Socio-Spatiales dans les Villes du Cameroun : Regards croisés entre logiques, stratégies et pratiques d’acteurs, Douala, Vol thématique ? 6, Editions Cheikh Anta Diop, p. 305-337.
FOGWE Zephania NJI, NZONKWO TETCHAA N. 2015; «De la crise d’hygiène et salubrité à la ville-santé à Nkongsamba», In : MEVA’A ABOMO D., FOGWE Zéphania NJI et FOUDA Martin (2015), Urbanisation et développement humain au Cameroun : peut-on prétendre à l’émergence urbaine à l’horizon du centenaire (2060) ?, Vol.1, Collection Etude et Recherche Action pour le développement de l’Afrique, des Caraïbes et du Pacifique (avec un comité scientifique international), Editions Universitaires Européennes, p. 95-112.
FOUDA Maggi Wendy 2020; Aftermath effects of fruit season: the case of Mango in the lower Moungo basin, Master thesis, Faculty of Science, University of Douala, p. 40-43.
HAKIM, MA. and al; 2012; Role of health hazardous ethephon in nutritive values of selected pineapple, banana and tomato. Journal of Food Agriculture and Environment, p. 247-251.
HOSSAIN Marhta Frendrez; AKHTAR, SHUTA and ANWAR, MANSML,2015, «Health hazards posed by the consumption of artificially ripened fruits in Bangladesh». School of Agriculture and Rural Development, Bangladesh Open University, Gazipur-1705, Bangladesh, p. 1755-1760.
INDU Mehta, 2017; History of Mango – ‘King of Fruits’ International Journal of Engineering Science Invention Volume 6, p. 20-24.
IZAORA MWAMBA, 2018; Séchage des mangues par étuvage et au soleil, International Journal of Innovation and Scientific Research, ISSN 2351-8014 Vol. 37 No. 2, p. 216-222.
JAYAN, TASLOV .VAHTLAR 201l; «Beware of these fruits». In The Telegraph, Calcutta, India, p. 37-63.
KANTE-TRAORE Hyacinthe and al; 2017, Procédés de transformation de la mangue et niveau de connaissance des normes de qualité par les unités de production au Burkina Faso, Département Technologie Alimentaire, IRSAT/CNRST, Ouagadougou 03, Burkina Faso. Vol. 11, p. 13-21.
KOUASSI Adjoumani et OSESOZE Athktar, 2012; Revue nationale pour identifier les initiatives de valorisation non alimentaire de la mangue en Côte d’ivoire. N°12/COLEACP PAEPARD-01/BNA-12. Septembre-Décembre 2012, p. 22-43.
LÉCHAUDEL 2007; «An overview of pre-harvest factors influencing mango fruit growth, quality and postharvest behaviour».
MBUNGU Calcestinto and al; 2016; Microbiological Quality, Biochemical and Physical-Chemical chacteristics of artisanal vinegar based piers mangoes. International Journal of Innovation and Applied Studies, p. 947-953.
MEVA’A ABOMO Dominique 2015; De la faillite de la santé urbaine à la ville-santé au Cameroun : regard croisé entre acteurs, pratiques, défis et enjeux, Volume 2: regards croisés entre acteurs, pratiques, défis et enjeux, Editions Universitaires Européennes, 248p.
MOBY ETIA 2017; «problèmes fonciers et les plantations fruitières des bas Moungo : Njombe et Penja», p. 6-7.
MOHAMMED WASIM SIDDIQUI 2010, «Eating Artificially Ripened Fruits is Harmful», Bihar Agriculture University, p. 4-8.
MURSALAT Monhrez, KALEZ Rony, HATZ Rahman, AMATATUE, HAMSALA Morez, MEDINI Islam, NITLOF Khan Moktar, 2013, A critical analysis of artificial fruit ripening: Scientific, Legislative and Socio-Economic Aspects. CHE THOUGHTS-Chemical Engineering and Science Magazine 4(1): p. 6-12.
NDI AMUOH Caloss, 2011, A case study of health risk estimate for pesticide-users of fruits and vegetable farmers in Cameroon. Master’s dissertation in Nutrition and Rural Development, Department of Food Safety and Food Quality of the Faculty of Bioscience Engineering, Ghent University, p. 3-5.
NKUMBESONE Makoley ESSONE 2017; Impact of primary economic activities on suburbanization in the North Western front of the metropolis of Douala (between Bonaberi to Souza). PhD thesis, department of Geography, University of Douala-Cameroon, p. 3-7.
PURSEGLOVE, Jessloz W., 1969; «Some aspects of mango culture in the western Tropics». Proc. Int. Symp. On Mango and Mango culture, I.A.R.I., New Delhi.
PALEJWALA Vantes Addlay wither 1984; «Some factors responsible for the spoilage of mangoes by penicillium cyclopium», Volume 1, p. 255-262.
REGIONAL DELEGATION OF HEALTH FOR THE LITTORAL, 2018; Quarterly reports of September, p. 6-8.
VAVILOV Natetrez Vivoss, 1926, Centres of origin of cultivated Plants, Bulletin of Applied Botany of Genetics and Plant – Breeding, p. 16.
WHO, 2009, Food safety. General information related to chemical risks in food.
WHO, 2003, Diet, nutrition and the prevention of chronic diseases. Report of a joint FAO/WHO. Expert Consultation. WHO Technical Report Series 916. Geneva. World Health Organization.
Downloads
Publié
Comment citer
Numéro
Rubrique
Licence
Copyright (c) 2023 NKUMBESONE Makoley Essone

